- Lumpectomy
- Mastectomy
- Modified Radical Mastectomy
- Radical Mastectomy
- Axillary Lymph Node Dissection
- Sentinel Lymph Node Biopsy
- Reconstructive Surgery
Lumpectomy
Lumpectomy
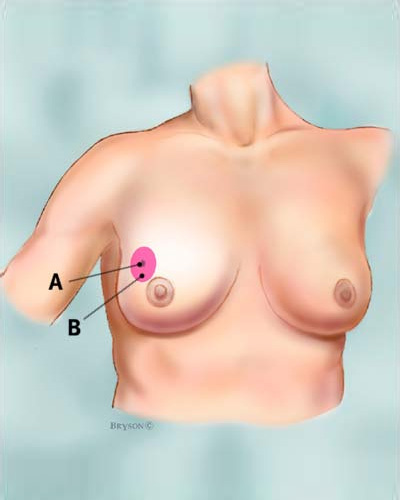
Lumpectomy is the removal of the breast tumor (the “lump”) and some of the normal tissue that surrounds it. Lumpectomy is a form of “breast-conserving” surgery. A Lumpectomy may also be referred to as a Partial Mastectomy. Technically, a lumpectomy is a partial mastectomy, because part of the breast tissue is removed. However, the amount of tissue removed can vary greatly. That is why it is important that you have a clear understanding of how much breast tissue may be removed during surgery and what kind of scar you will have. Dr. Zadeh will go through the procedure with you in detail and answer any questions you may have.
Mastectomy
Mastectomy is the removal of the whole breast. The main types of mastectomy are: “simple” or “total” mastectomy, modified radical mastectomy, and radical mastectomy.
Total Mastectomy
“Simple” or “total” mastectomy
In a “simple” or “total” mastectomy the entire breast tissue is removed, however an axillary lymph node dissection (removal of lymph nodes in the underarm area) is not performed. Unlike a radical mastectomy, no muscles are removed from beneath the breast.
Who usually gets a “simple” or “total” mastectomy?
A “simple” or “total” mastectomy is appropriate for women with multiple or large areas of ductal carcinoma in situ (DCIS) and for women seeking prophylactic mastectomies, that is, breast removal in order to prevent any possibility of breast cancer occurring.
Modified Radical Mastectomy
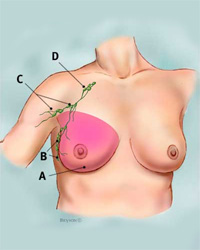
In a Modified Radical Mastectomy the entire breast tissue is removed along with the lymph nodes of the underarm in what is termed an Axillary Lymph Node Dissection (B and C in the figure). The muscles of the chest wall are spared.
Modified radical mastectomy
Who usually gets a Modified Radical Mastectomy?
Most people with invasive breast cancer who decide to have mastectomies will receive modified radical mastectomies so that the lymph nodes can be examined. Examining the lymph nodes helps to identify whether cancer cells may have spread beyond the breast. Dr. Zadeh employ’s a newer modality to evaluate the lymph nodes called a Sentinel Node Biopsy. This method of lymph node evaluation may save the patient a full axillary lymph node dissection and the risks that go along with it.
Back to Top
Radical Mastectomy
Radical mastectomy
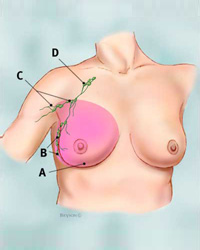
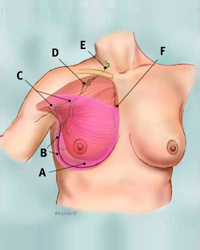
Radical mastectomy is the most extensive type of mastectomy and involves removal of the entire breast along with all of the regional axillary lymph nodes. The chest wall muscles underneath the breast are also removed.
Who usually gets a Radical Mastectomy?
While at one time the radical mastectomy was the most common procedure performed for breast cancer, today it is mostly of historical value. Recent studies have shown that in most cases modified radical mastectomy, and even breast conserving therapy has proven to be just as effective and less disfiguring in the treatment of breast cancer. Radical Mastectomy is now reserved for those rare cases in which the breast cancer has spread to the chest muscles under the breast.
Back to Top
Axillary lymph node dissection
When breast cancer invades beyond the breast, the first site of spread is to the regional lymph nodes. These lymph nodes are located in the underarm and are called the axillary lymph nodes. To determine if the breast cancer has spread to the axillary lymph nodes, some of these lymph nodes may be removed during surgery and looked at under the microscope by the pathologist. The status of the axillary lymph nodes is the most important factor in staging and determining treatment and outcomes in breast cancer. When the lymph nodes contain cancer cells, there is a higher chance that cancer cells have also spread through the bloodstream to other parts of the body.
As noted above, axillary lymph node dissection is part of a radical or modified radical mastectomy procedure. It may also be done along with a breast-conserving procedure, such as a lumpectomy. An adequate axillary lymph node dissection contains at least 12 lymph nodes which can be examined by the pathologist.
If you undergo an axillary lymph node dissection as part of your procedure, it is very likely that you will have a temporary drain inserted to prevent fluid collection post-operatively. Click here for instructions on how to care for the drain.
Information for arm exercises after an axillary lymph node dissection can be found here
Sentinel lymph node biopsy
Although axillary lymph node dissection is a safe operation with low rates of complications, newer technology has become available in recent years that enable surgeons to minimize the number of unnecessary axillary dissections performed, along with the complications associated with those procedures. This new method, called a Sentinel Lymph Node biopsy is a way of learning if cancer has spread to lymph nodes without removing all of them.
In this procedure a radioactive substance and/or a blue dye is injected into the tumor or the area around it prior to surgery. The lymphatic system of the breast will carry these substances into the sentinel node, which is the first lymph node in the region to receive the lymphatic drainage. Therefore, if cancer cells have spread beyond the breast into the lymphatic system this sentinel lymph node is the one most likely to contain the cancer cells. A special device is used to detect the radioactive substance within the sentinel node or alternatively, the sentinel node can be identified by its blue coloration after it has taken up the injected dye. Once identified the sentinel lymph node is then removed and sent to pathology for analysis.
If there is no cancer in the sentinel node, it’s very unlikely that the cancer has spread to other lymph nodes, and no further lymph node surgery is needed. The patient can avoid the potential complications associated with a full axillary lymph node dissection.
If the sentinel node is positive for cancerous cells, then a full axillary lymph node dissection is required to assess lymph node status.
Sentinel Lymph Node biopsy requires a great deal of skill and experience. Dr. Zadeh performs Sentinel Lymph Node biopsies for both breast conserving procedures and for mastectomies.
Reconstructive Surgery
After having a mastectomy, a woman may want to consider having the breast mound rebuilt; this is called breast reconstruction. These procedures are not done to treat cancer but to restore the breast’s appearance after surgery. If you are going to have breast surgery and are thinking about having reconstruction, it is important to consult with a plastic surgeon who is an expert in breast reconstruction before your surgery.
Decisions about the type of reconstruction and when it will be done depend on each woman’s medical situation and personal preferences. You may have a choice between having your breast reconstructed at the same time as the mastectomy (immediate reconstruction) or at a later time (delayed reconstruction). There are several types of reconstructive surgery. Some use saline (salt water) or silicone implants, while others use tissues from other parts of your body (autologous tissue reconstruction). Your plastic surgeon will help decide which form of reconstruction is most appropriate for you.
If you are considering breast reconstruction, you may find it helpful to talk with other women who have had the type of reconstruction you might be considering. Our office can help put you in contact with willing volunteers.

Click to read blog post on breast cancer risk and detection